Health-related Resources for people with IDD and Their Supporters
 Health-related Resources for People with IDD and Their Supporters
Health-related Resources for People with IDD and Their Supporters
By Craig Escudé, MD, FAAFP, FAADM
Published by EP Magazine | January 2023
 With significant health disparities noted in people with IDD, it is important that people with intellectual and developmental disabilities (IDD), their supporters, and healthcare providers educate themselves on the different health risks that are more commonly seen in people with IDD and about what can be done to prevent serious complications. Supporters and healthcare providers are often challenged in finding helpful information related to healthcare for people with IDD. As a physician who started practicing in this field in the 1990s, finding clinically relevant information about healthcare for people with IDD was challenging. Fortunately, over the past several years, more resources have been developed that relate specifically to healthcare issues and improving health equity for people with IDD. In this article, you’ll find a listing of websites, tools, and training available to provide information and guidance to you, whether a family member, paid supporter, healthcare provider, or person with IDD.
With significant health disparities noted in people with IDD, it is important that people with intellectual and developmental disabilities (IDD), their supporters, and healthcare providers educate themselves on the different health risks that are more commonly seen in people with IDD and about what can be done to prevent serious complications. Supporters and healthcare providers are often challenged in finding helpful information related to healthcare for people with IDD. As a physician who started practicing in this field in the 1990s, finding clinically relevant information about healthcare for people with IDD was challenging. Fortunately, over the past several years, more resources have been developed that relate specifically to healthcare issues and improving health equity for people with IDD. In this article, you’ll find a listing of websites, tools, and training available to provide information and guidance to you, whether a family member, paid supporter, healthcare provider, or person with IDD.
Books
Clinical Pearls in IDD Healthcare provides easy-to-understand and clinically relevant information to clinicians and supporters of people with IDD. The book is centered on “clinical pearls,” which are small bits of free-standing, clinically relevant information based on experience or observation. They are part of the vast domain of experience-based medicine and can be helpful in dealing with clinical problems for which controlled data do not exist.
You will find 1-2 page documents covering 55 health-related conditions commonly seen in people with IDD. Topics include medical causes of adverse behavior, sexuality, quality of life, end-of-life care, dental care, polypharmacy, common preventable cause of illness, aging with IDD, and much more. The guide is used by physicians, supporters, nurses, and family members to gain an understanding of the many health issues that are more common in people with IDD. For family members, it can be helpful for self-education but also as a means to provide concise information to physicians who may appreciate additional clinical details related to IDD healthcare.
Electronic Learning Courses
For clinicians looking to receive additional training in IDD Healthcare, the Curriculum in IDD Healthcare is a web-based Continuing Medical Education-approved eLearning course that teaches the fundamentals of IDD healthcare that were likely not taught in clinical training programs. It’s a 6 module, self-paced course that has been studied and shown to significantly improve clinicians’ clinical confidence in providing healthcare to people with IDD. It’s currently used in medical and nursing schools and by practicing clinicians throughout the United States.
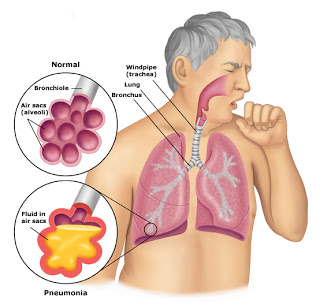
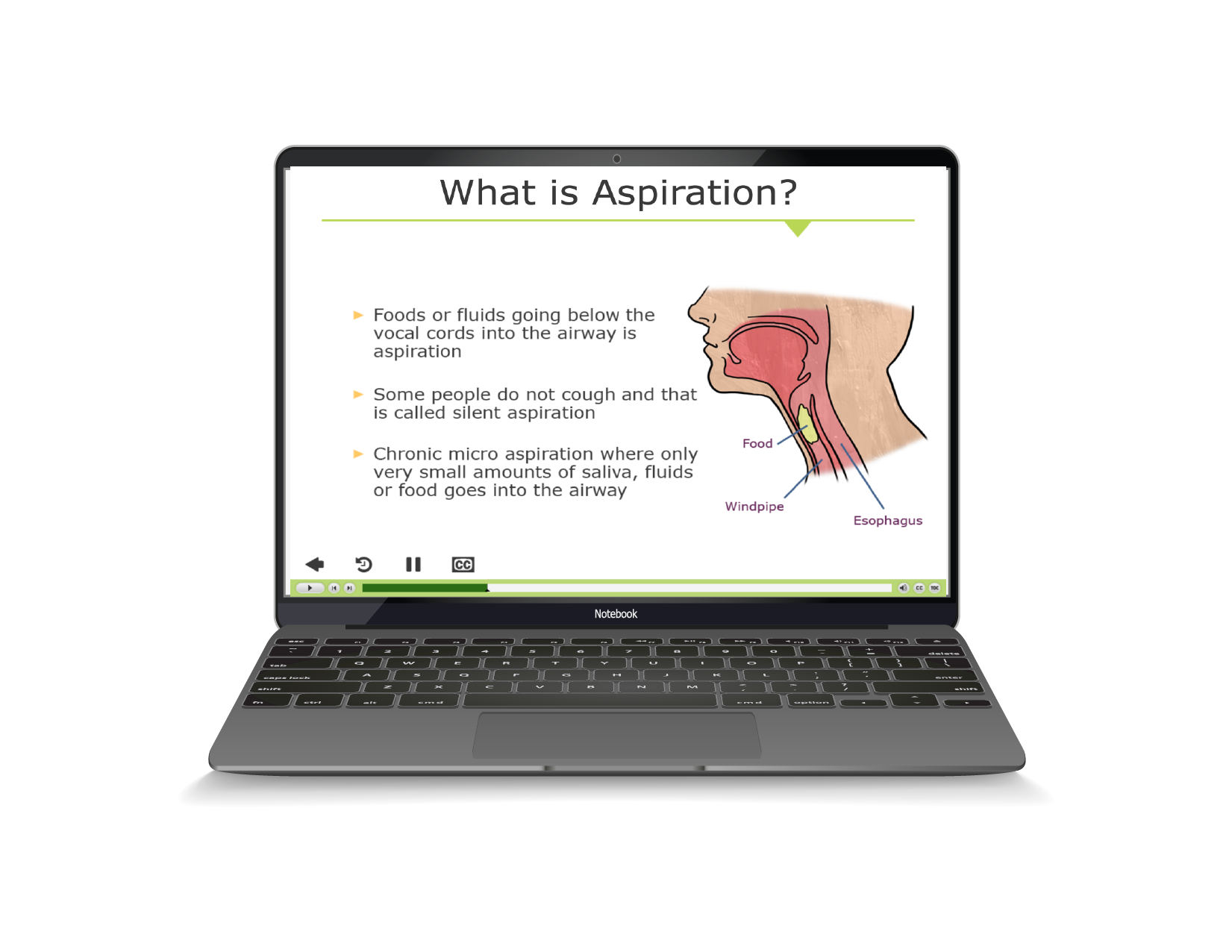
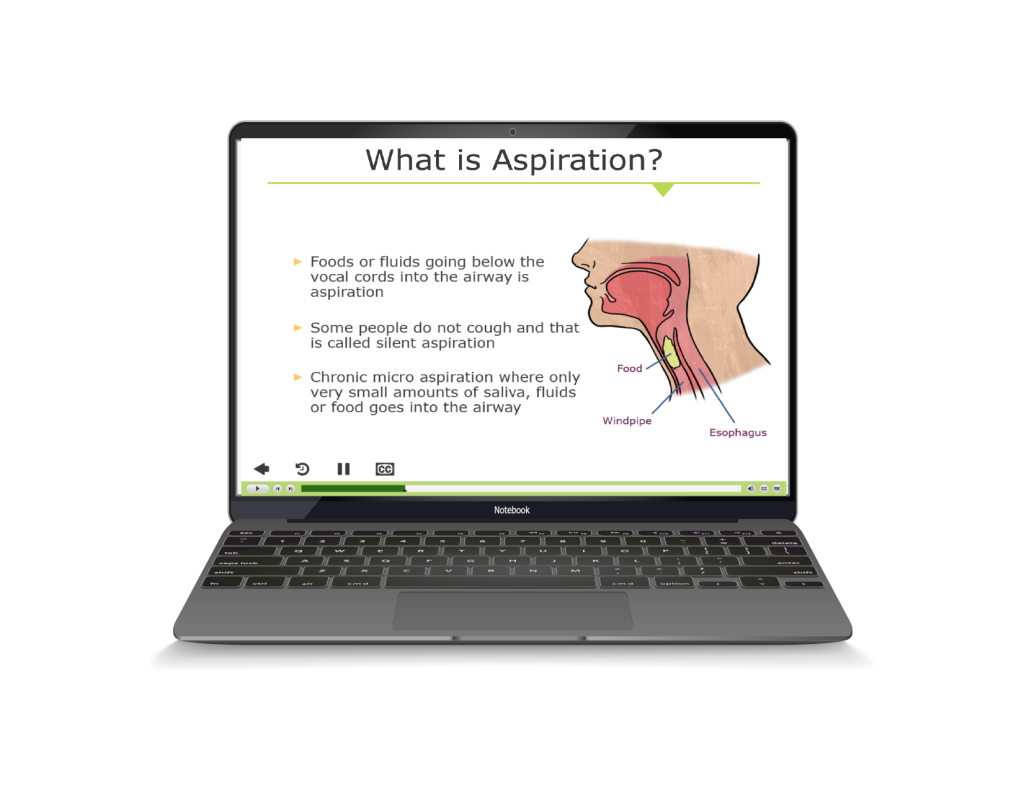
The Fatal Five eLearning courses are excellent programs that teach learners about the top preventable causes of illness and death in people with IDD. The specific topics covered in these 7-module courses include discussions about aspiration, dehydration, seizures, bowel obstruction, sepsis, and gastroesophageal reflux, as well as a discussion on knowing when to act to avoid serious complications. The Fatal Five Fundamentals is geared to teach direct support professionals and family members about these topics. The Fatal Five Advanced course teaches about the same conditions at a more clinical level, which is great for nurses.
Websites
Special Olympics has a webpage dedicated to health resources for people with IDD. Topics include Health Promotion, Fitness, Health Smiles (dentistry), and many other health and wellness resources.
The Eunice Kennedy Shriver National Institute of Child Health and Human Development has an extensive list of IDD health resources for patients, healthcare providers, and researchers. You’ll find general and condition-specific information, including links to related entities such as the Association for University Centers on Disabilities.
The Vanderbilt Kennedy IDD Toolkit is an excellent resource guide for clinicians and others relating to several common genetic conditions often associated with IDD. In addition to general guidance, there is specific guidance for health screening about conditions like Autism, Down Syndrome, Fragile X, Prader-Willi, and other conditions, as well as a number of valuable resources relating to topics such as informed consent, communication, and behavioral health.
Organizations
There are two organizations for healthcare providers that offer resources online and provide educational opportunities at their annual conferences. The American Academy of Developmental Medicine and Dentistry focuses on physicians and dentists and the Developmental Disabilities Nurses Association for nurses. Both organizations are excellent resources where providers can enhance their skills and knowledge in providing IDD healthcare and collaborate with others in the field.
Several organizations provide valuable information about specific genetic conditions and syndrome, including the Prader-Willi Syndrome Association, the National Association for Down Syndrome, the National Autism Association, the Autism Society of America, the National Fragile X Foundation, the Angelman Syndrome Foundation, and others. Many of these societies have information tailored to supporters, family members, healthcare providers, and researchers relating to their specific syndrome.
Finding Additional Resources
The internet is filled with resources, but not all are what I’d call “good.” And some contain misinformation or are more based on people’s opinions rather than what is generally considered acceptable and reliable health-related information. When looking for resources, I’d recommend going to websites that are from known entities such as well-known hospital systems, governmental agencies like the CDC and the NIH, or official websites for whatever you are looking for. I also recommend reaching out to people you know in your community to see what resources they recommend. Talk to trusted physicians and nurses or call your local hospital to see if there might recommend a particular resource.
Final Thoughts
I’m sure that there are many excellent resources I have left out. But hopefully, the ones listed here will be useful to many. Educating ourselves about our health and the health of the people we support can help us make better-informed decisions, which can dampen the anxiety and fear we might face when dealing with health challenges.
About the author:
Dr. Craig Escudé is a board-certified Fellow of the American Academy of Family Physicians and the American Academy of Developmental Medicine and is the President of IntellectAbility. He has more than 20 years of clinical experience providing medical care for people with IDD and complex medical and mental health conditions serving as medical director of Hudspeth Regional Center in Mississippi for most of that time. While there, he founded DETECT, the Developmental Evaluation, Training, and Educational Consultative Team of Mississippi. He is the author of “Clinical Pearls in IDD Healthcare” and developer of the “Curriculum in IDD Healthcare,” an eLearning course used to train clinicians on the fundamentals of healthcare for people with IDD.


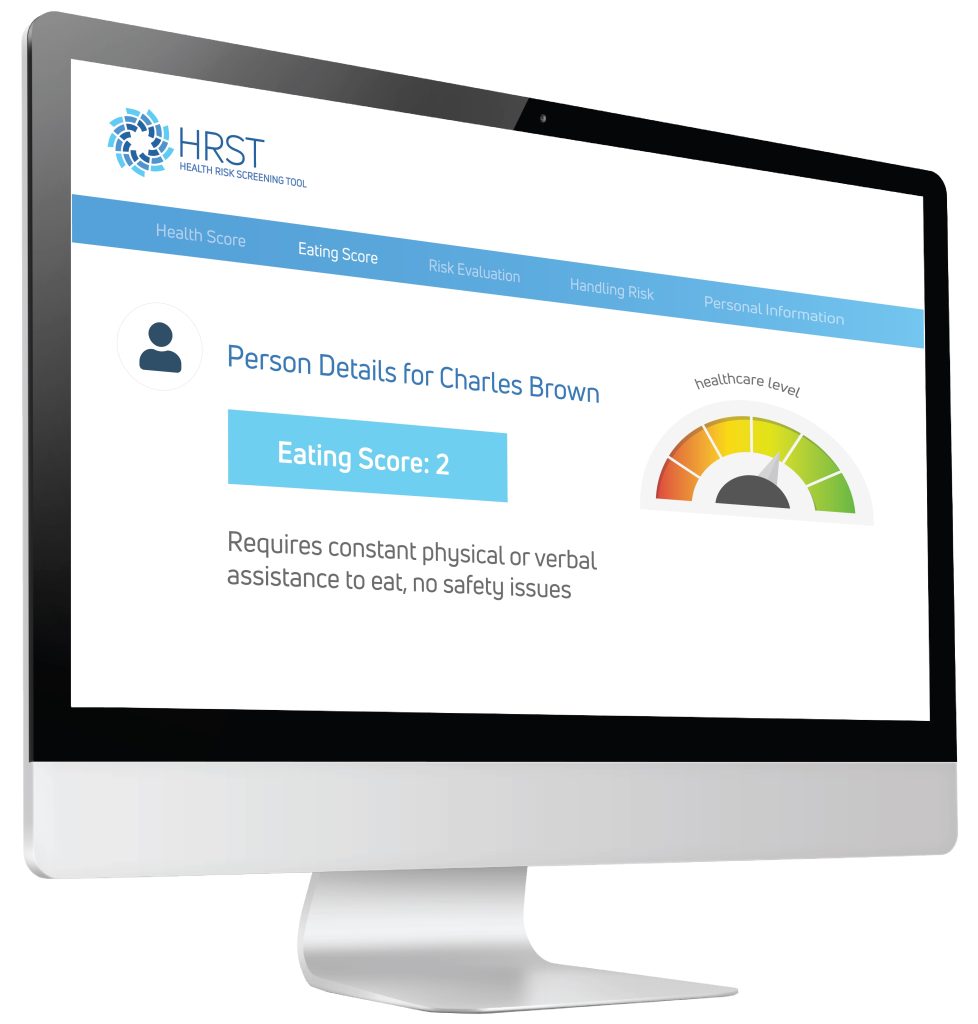 Using the information provided by the case manager, the HRST recognized the possibility of an undiagnosed gastrointestinal condition as the potential cause of Jerome’s behavioral symptoms and produced a “service consideration” suggesting the need for clinical follow-up to rule out Gastroesophageal Reflux Disease (more commonly known as GERD).
Using the information provided by the case manager, the HRST recognized the possibility of an undiagnosed gastrointestinal condition as the potential cause of Jerome’s behavioral symptoms and produced a “service consideration” suggesting the need for clinical follow-up to rule out Gastroesophageal Reflux Disease (more commonly known as GERD).
 The
The